The Andes virus (ANDV) is a highly lethal orthohantavirus belonging to the family Hantaviridae, first identified in 1995 in Chile and Argentina, where it remains endemic across Patagonian and Andean ecosystems. It is primarily harbored by the long-tailed pygmy rice rat (Oligoryzomys longicaudatus), which sheds the virus asymptomatically through urine, feces, and saliva. Humans typically become infected by inhaling aerosolized rodent excreta, though ANDV holds the unique and alarming distinction of being the only hantavirus capable of person-to-person transmission — a property demonstrated during multiple outbreaks, including a 2018–2019 cluster in Chubut, Argentina, where the reproduction number reached 2.12 before isolation measures were applied. Upon infection, ANDV targets pulmonary microvascular endothelial cells via β3-integrin receptors, triggering a non-cytopathic but devastating cascade of vascular hyperpermeability, cytokine storm, and pulmonary edema that defines Hantavirus Cardiopulmonary Syndrome (HCPS) — a disease carrying a case fatality rate of approximately 40%. There is currently no approved antiviral treatment or licensed vaccine; management relies entirely on intensive supportive care, with extracorporeal membrane oxygenation (ECMO) representing the most effective rescue intervention in severe cases. Given its pandemic potential, ANDV is classified as a WHO priority pathogen and remains an active subject of vaccine and therapeutic research.
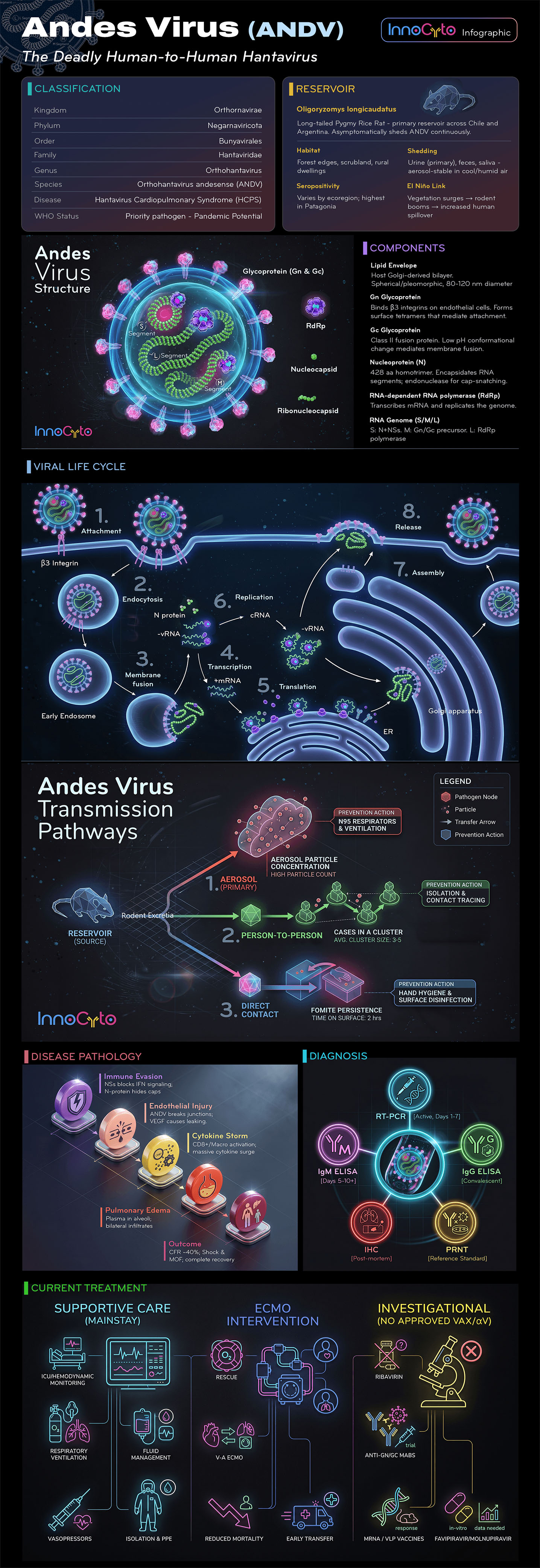
The Deadly Human-to-Human Hantavirus
| Rank | Name |
|---|---|
| Kingdom | Orthonavirae |
| Phylum | Negarnaviricota |
| Order | Bunyavirales |
| Family | Hantaviridae |
| Genus | Orthohantavirus |
| Species | Orthohantavirus andesense (ANDV) |
| Disease | Hantavirus Cardiopulmonary Syndrome (HCPS) |
| WHO Status | Priority pathogen – Pandemic Potential |
Oligoryzomys longicaudatus Long-tailed Pygmy Rice Rat – primary reservoir across Chile and Argentina. Asymptomatically sheds ANDV continuously.
Forest edges, scrubland, rural dwellings
Urine (primary), feces, saliva – aerosol-stable in cool/humid air
Varies by ecoregion; highest in Patagonia
Vegetation surges → rodent booms → increased human spillover
Lipid Envelope: Host Golgi-derived bilayer. Spherical/pleomorphic, 80–120 nm diameter.
Gn Glycoprotein: Binds β3 integrins on endothelial cells. Forms surface tetramers that mediate attachment.
Gc Glycoprotein: Class II fusion protein. Low pH conformational change mediates membrane fusion.
Nucleoprotein (N): 428 aa homotrimer. Encapsidates RNA segments; endonuclease for cap-snatching.
RNA-dependent RNA Polymerase (RdRp): Transcribes mRNA and replicates the genome.
RNA Genome (S/M/L): S: N + NSs; M: Gn/Gc precursor; L: RdRp polymerase.
Reservoir (Source): Rodent Excreta
Immune Evasion: NSs blocks IFN signaling; N-protein hides caps.
Endothelial Injury: ANDV breaks junctions; vEGF causes leaking.
Cytokine Storm: CD8+/Macrophage activation; massive cytokine surge.
Pulmonary Edema: Plasma in alveoli; bilateral infiltrates.
Outcome: Case Fatality Rate ~40%; Shock & Multi-organ failure; complete recovery possible.
| Method | Window |
|---|---|
| RT-PCR | Active infection, Days 1–7 |
| IgM ELISA | Days 5–10+ |
| IgG ELISA | Convalescent |
| IHC | Post-mortem |
| PRNT | Reference Standard |
Contact us for expert support.
Andes Virus Glycoprotein Gn Head Neutralizing Antibody, clone ANDVAB
Andes Virus Glycoprotein Gn Head Neutralizing Antibody, clone ANDVBB
Andes Virus Glycoprotein Gn/Gc Neutralizing Antibody, clone ANDVCB
Andes Virus Glycoprotein Gn Ectodomain Neutralizing Antibody, clone ANDVDB
Andes Virus Glycoprotein Gn Ectodomain Neutralizing Antibody, clone ANDVEB
Andes Virus Glycoprotein Gn Head (C-His)
Andes Virus Glycoprotein Gc (C-His)
Andes Virus Glycoprotein Gc (H953F) (C-His)
Andes Virus Glycoprotein Gn Head/Gc Complex (C-His)
Andes Virus Glycoprotein Gn Head/Gc (H953F) Complex (C-His)
Andes Virus Gn Base Protein (C-His)